[Paper] The Psychological Impact of COVID-19 State of Emergency on Non-Regular Workers: A Nationwide Follow-Up Survey in Japan
![[Paper] The Psychological Impact of COVID-19 State of Emergency on Non-Regular Workers: A Nationwide Follow-Up Survey in Japan](https://humedit.com/wp-content/uploads/paper.jpg)
Table of Contents
- Summary
- Background
- Methods
- Results
- Discussion
- Table 1: Baseline Characteristics Before and After Propensity Score Matching
- Figure 3: Box Plots of Changes in CES-D Scores and Health-Related Utility, and Background Diagrams of Unemployment Experience in the Persistent and Non-Persistent Groups
- Table 2: Multiple Regression Model of Socioeconomic Indicators and Changes in CES-D Scores (N = 2351)
- Conclusion
Summary
Background
The COVID-19 pandemic has caused mental health issues and increased unemployment due to the economic downturn. This study aimed to assess the psychological impact of the state of emergency. It estimated changes in mental health, quality of life (QOL), and unemployment experience among general workers during the initial COVID-19 outbreak in Japan.
Methods
The authors conducted a nationwide follow-up survey. Using the internet, they surveyed general workers aged 15-59 in Japan from March 26 to April 6, 2020, and from June 26 to July 2, 2020. The survey items targeted employment status and socioeconomic factors and utilized the Epidemiological Research Center's Depression Scale (CES-D) and the EQ-5D-5L to assess depression and health-related quality of life (HR-QOL). Using propensity score analysis, they analyzed the differences in outcomes between regular and non-regular employees. Multiple linear regression analysis was conducted to examine the relationship between unemployment and CES-D scores.
Results
The analysis included 2,351 subjects. Changes in both CES-D scores and utility did not show significant differences between the two groups. However, a significant difference was observed regarding the unemployment rate associated with higher CES-D scores.
Conclusion
This study demonstrated that the mental health of non-regular workers was not negatively affected after the COVID-19 state of emergency in Japan. Unemployment is an important factor affecting the mental health of general workers.
Keywords: COVID-19, general workers, mental health, propensity score analysis, QOL, job security, unemployment, web survey
Background
The coronavirus disease has had a significant impact on global public health and has spread worldwide. As of August 3, 2020, 17,918,582 cases of COVID-19 have been confirmed, and 686,703 deaths have been reported globally[1]. Many countries have temporarily succeeded in curbing the spread of COVID-19 by closing international borders and implementing nationwide lockdowns. However, these measures have reduced the workforce across economic sectors, resulting in many job losses[2].
In Japan, a state of emergency was declared on April 7, 2020, in seven prefectures, including Tokyo and Osaka. Due to a surge in "untraceable" new infections, the emergency was expanded nationwide, and 13 prefectures were designated as "special alert areas" on April 16. In response to the emergency declaration, the government urged citizens to refrain from going out, maintain social distancing, stay home, comply with travel restrictions, and closed non-essential businesses for about a month[3,4].
The COVID-19 pandemic has led to mental health issues and increased unemployment due to the economic downturn. A large cross-sectional study conducted in China showed that being employed reduced the risk of depression, anxiety, and insomnia[5]. Several studies have reported that during the early stages of the COVID-19 outbreak, the rates of depression and anxiety among Spaniards were 18.7% and 21.6%, respectively. Spanish adults confined by COVID-19 movement restrictions showed an inverse correlation between current physical activity and perceived anxiety and mood[6,7]. The Organisation for Economic Co-operation and Development (OECD) noted that the unemployment rate increased by 2.9% reflecting the impact of containment measures due to COVID-19[2]. Recently, a report by the Japanese government indicated that during the COVID-19 crisis, the mental health of the unemployed and non-regular workers might be particularly vulnerable[8].
In Japan, the number of non-regular workers has been increasing. Early employment includes part-time, temporary, and fixed-term employment, accounting for 22% of male and 53% of female paid employment in 2020[9]. Job insecurity has negative effects on the mental health of non-regular workers, and unemployment was associated with psychological conditions such as depression, anxiety, and poor health outcomes. Previous studies suggested that precarious employment among middle-aged Japanese men was associated with a twofold risk of severe psychological distress[10]. Additionally, different employment situations in East Asia were associated with the onset of severe depressive symptoms[11,12]. Poor mental health conditions, including depression, are well-known independent risk factors for suicide and are associated with a decreased quality of life compared to healthy subjects[13,14].
The current focus on the COVID-19 outbreak includes not only the medical outcomes of infected patients but also the mental health of patients and the general population. Therefore, it is meaningful to investigate changes in mental health and quality of life during the COVID-19 crisis. The relationship between job security and mental health issues after the state of emergency in Japan has not yet been examined. This study aims to assess the psychological impact of the state of emergency. It estimated changes in mental health, quality of life (QOL), and unemployment experience among general workers during the initial COVID-19 outbreak in Japan.
Methods
Study Design and Data Collection
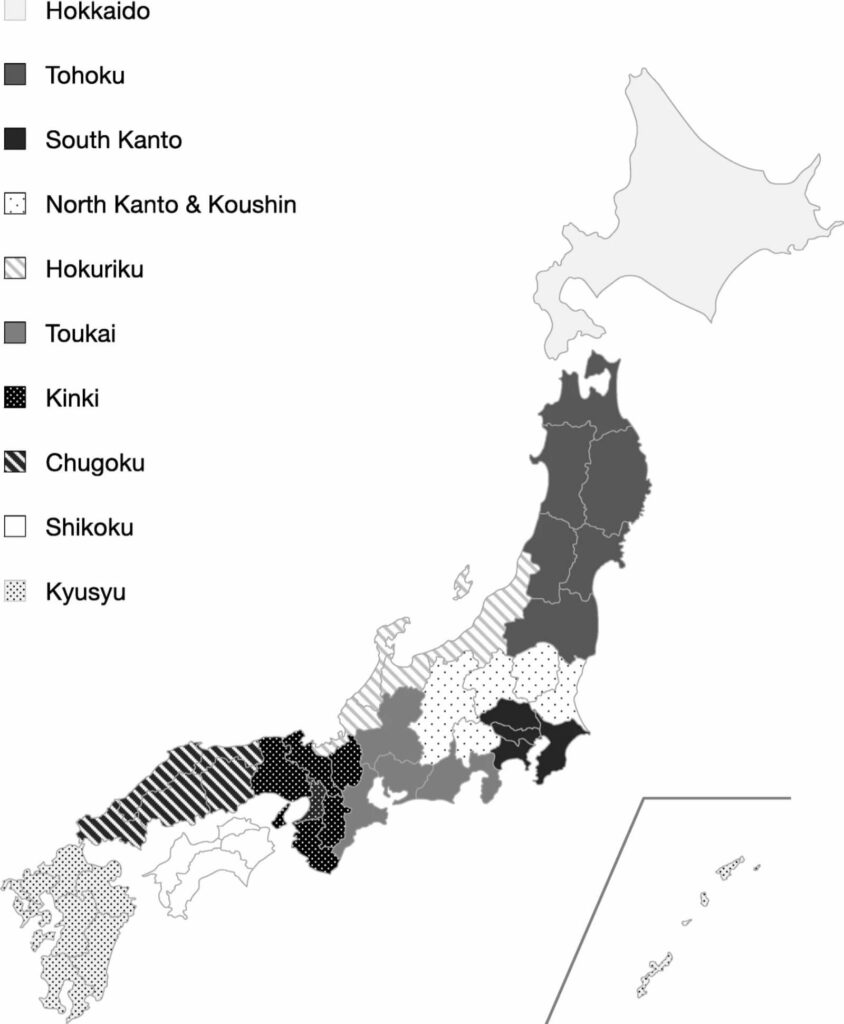
This nationwide survey targeted general workers in Japan aged 15-59 and was conducted online through a platform with over 2 million candidates. It was managed by Cross Marketing Inc. (Tokyo), a company specializing in questionnaire surveys. The initial survey was conducted from March 26 to April 6, 2020, before the COVID-19 state of emergency was declared. The follow-up survey was conducted from June 26 to July 2, 2020, after the state of emergency was lifted, targeting the same cohort of respondents. The initial survey continued until data was collected from 3,000 respondents, and the follow-up survey aimed to include 70% of the initial cohort based on the general response rate for web-based surveys. The initial survey ensured a representative sample of the Japanese population concerning age, gender, and residential area. The residential areas in Japan were divided into 10 regions (Figure 1). Participants in this study were not offered any incentives or rewards.
Survey Operational Status
The authors defined working status into the following four types, and subjects selected their status during self-reporting. A regular employee refers to a company employee who is directly employed by the employer, with guaranteed lifetime employment until retirement.
Non-Regular Employees
Part-time workers, temporary agency workers, and contract or commissioned employees who have entered into a fixed-term employment contract.
Public Servants
Public servants employed by national or local government authorities and those incorporated into non-profit organizations.
Self-Employed
Self-employed individuals such as sole proprietors and freelancers. The study population consisted of workers employed by general companies. Public servants were excluded because their employment is guaranteed until retirement in Japan. Additionally, self-employed individuals were excluded as they are not employees.
Figure 1: Ten Regions of Japan
Socioeconomic and Medical Conditions
The questionnaire covered age, gender, region, marital status, children, cohabiting family members, education, industry, company size, personal income, family income, average monthly overtime hours, union membership, head of household, exercise, smoking history, drinking history, commute time, and average sleep duration.
Additionally, information on the history of physical and mental illnesses such as heart disease, cerebrovascular disease, cancer, Alzheimer's disease, chronic pain conditions, epilepsy, and depression was collected in accordance with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)[15]. In this analysis, the number of diseases was defined as a major factor. The stress coping ability was measured using the Japanese version of the Sense of Coherence (SOC) scale, with final scores ranging from 13 to 91. This scale includes 13 items, with higher scores indicating better stress coping ability[16].
Outcomes
In both the first and second surveys, the severity of depressive symptoms and HR-QOL were assessed. Depressive symptoms were measured using the Japanese version of the CES-D. This scale consists of 20 items, and participants were asked to rate the frequency of symptoms associated with depression they experienced over the past week. The CES-D score ranges from 0 to 60, with scores over 16 typically indicating depressive symptoms. The CES-D has high sensitivity, specificity, and internal consistency for identifying the risk of depression[17].
The 5-dimension EQ-5D-5L instrument was used to assess respondents' HR-QOL. The EQ-5D-5L consists of five items: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, across five levels. The resulting scale, based on general preference, reflects subjective values assigned to specific health-related outcomes ranging from -0.025 to 1, with 0 indicating death and 1 indicating perfect health according to the Japanese value set. This is referred to as utility weighting[18].
The differences in CES-D scores and utility values between the two time frames were defined as outcomes in this analysis. Additionally, unemployment experience during the emergency in the second survey was also investigated.
Statistical Analysis
Propensity score matching was performed to adjust for confounding factors between the persistent and non-persistent groups and to evaluate outcomes[19]. The propensity scores were estimated using a multiple logistic regression model with socioeconomic factors, comorbidities, baseline CES-D scores, and clinical indicators such as utility. Based on the propensity scores, nearest neighbor matching was performed without replacement, in a 1:1 ratio using a caliper of 0.2 standard deviations of the estimated propensity scores. For matched subjects, the absolute standardized differences of means and proportions of these variables were used to verify balance in propensity scoring between the two groups. In the matched cohort, changes in CES-D scores, utility changes, and unemployment experience rates between regular and non-regular employees were compared. Pearson's chi-squared test was used to compare categorical variables, and Student's t-test was used to compare continuous variables. Finally, the psychological impact of unemployment on changes in CES-D scores was evaluated. Multiple linear regression analysis was performed to identify determinants of the changes. Independent variables used in the analysis included working status, unemployment experience, gender, age, number of comorbidities, region, marital status, personal income, family income, average daily working hours, union membership, head of household, exercise, smoking, drinking, average sleep duration, SOC score, and baseline CES-D score. Categorical and ordinal variables were converted to dummy variables. The authors examined the interaction between working status and unemployment experience to assess the extent of psychological impact in the two groups.
All statistical tests were two-sided, and a p-value of less than 0.05 was considered significant. All analyses were conducted using STATA 16.1 (StataCorp LP, College Station, TX, USA).
Results
Data Collection
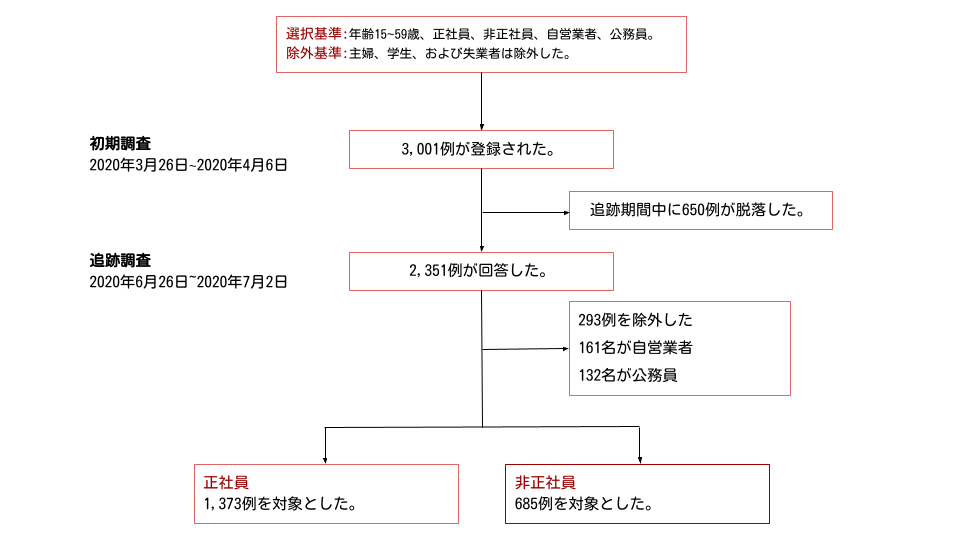
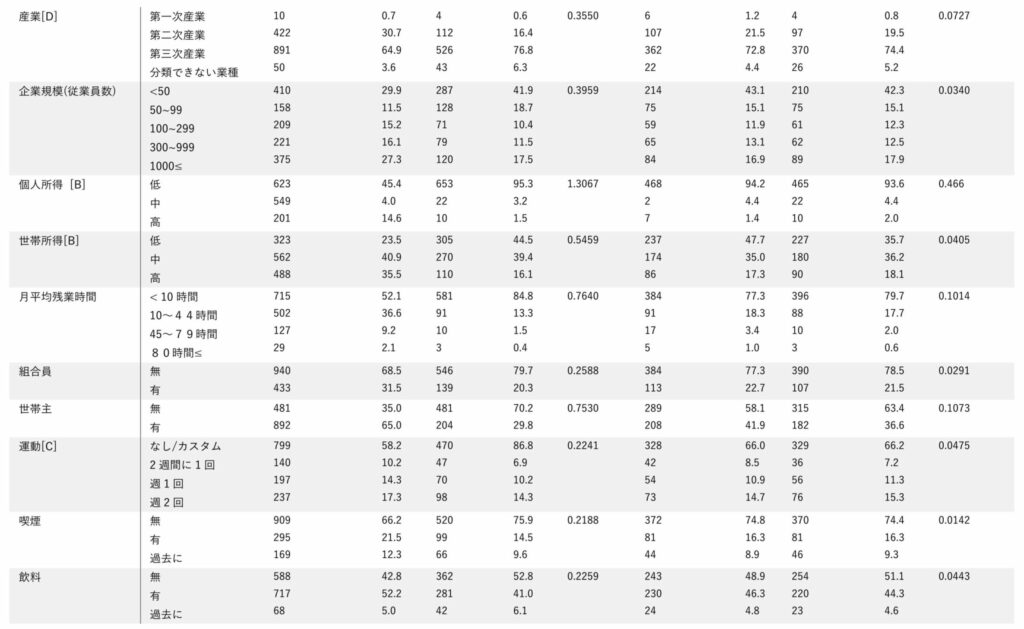
In the initial survey, data was collected from 3,001 subjects (excluding housewives, students, and the unemployed), and 2,351 subjects responded to the follow-up survey. Subsequently, 161 self-employed individuals and 132 public servants were excluded from the analysis. Finally, 1,373 regular employees and 685 non-regular employees were included in the propensity score matching for regular and non-regular employees (Figure 2).
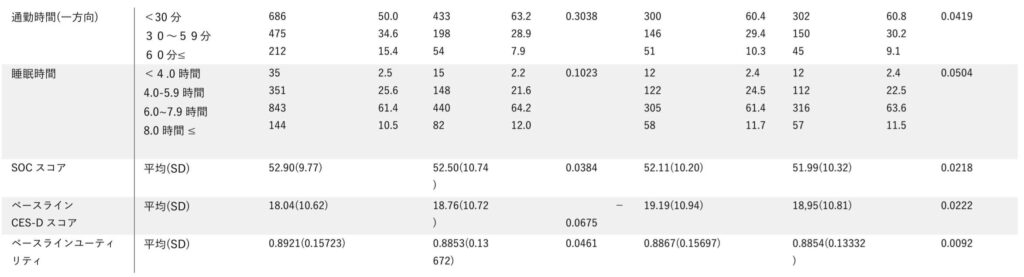
Propensity Score Analysis
Propensity score matching identified 497 cases from both the non-persistent and persistent groups. Therefore, a total of 994 subjects were included in the subsequent analysis. Table 1 shows the differences in baseline characteristics between the non-persistent and persistent groups before and after matching. All baseline variables included in the model were well-balanced within the standardized difference range or close to 0.1 after matching. The c-statistic for the propensity score was estimated at 0.862, ranging from 0.846 to 0.878, indicating good discrimination between the two groups. Data with no missing values were collected through the web survey. Figure 3 compares changes in CES-D scores, changes in utility, and unemployment rates. The change in CES-D scores was estimated at -0.706 for regular employees and -0.575 for non-regular employees (p = 0.807). There was no significant difference in utility changes between the two groups (persistent 0.014 vs. non-persistent 0.009, p = 0.533). However, there was a significant difference in unemployment rates, with data showing agreement (persistent 7.20% vs. non-persistent 11.47%, p = 0.022); the unemployment risk ratio was estimated at 1.583 (95% confidence interval = 1.063–2.358).
Figure 2: Flowchart of Study Participants
Multiple Regression Analysis
The results of the multiple regression analysis shown in Table 2 indicated that unemployment experience was a factor associated with an increase in CES-D scores (p = 0.003). There was no significant interaction between working status and unemployment (p = 0.340). Having two or more comorbidities (p = 0.044) and an average daily working time of 10-12 hours (p = 0.027) were associated with an increase in CES-D scores. Notably, higher SOC scores (p < 0.001), being married (p = 0.032), and baseline CES-D scores (p < 0.001) were associated with lower CES-D scores.
Discussion
The physiological impact of the COVID-19 outbreak is a global concern. This study investigated changes in CES-D scores, health-related utility, and unemployment among general workers during the COVID-19 state of emergency, based on data from a nationwide web-based questionnaire in Japan. After matching the background of the subjects, there were no statistically significant differences in these scores. However, unemployment in the non-persistent group was statistically higher than in the persistent group, even after adjusting for baseline factors. The findings suggest that employment conditions worsened after the emergency, especially for non-regular workers. Unemployment was found to deteriorate the psychological state of general workers in Japan.
Several studies have demonstrated predictors associated with increased depression and anxiety. In Japan, a cohort study conducted by Sairenchi et al. [20] revealed that SOC could predict the onset of depression among Japanese workers. Another study [21] reported that increased SOC might reduce negative work stress responses and subjective symptoms in general workers. Recently, a large cross-sectional study by Kikuchi et al. [22] found that Japanese workers with long overtime hours showed significantly higher anxiety and depression than those with fewer overtime hours, for both men and women. Furthermore, studies in Korea suggested that head of household status, gender, and unstable employment were associated with the onset of severe depressive symptoms [11].
The propensity score analysis adjusted for these factors between the persistent and non-persistent groups. Although there were no statistically significant differences in CES-D scores between the two groups, slight improvements were observed in both groups' scores. Non-regular workers reported higher unemployment rates compared to regular contract workers, but our data did not observe a significant impact on mental health. The results did not confirm the hypothesis regarding HR-QOL. However, since the EQ-5D-5L includes dimensions of anxiety/depression, deteriorating psychological states may affect HR-QOL. We believed that the increase in adverse mental health impacts would lower the HR-QOL of non-regular workers. Job security is a crucial factor in maintaining the mental health of non-regular employees. The increase in unemployment rates could potentially raise suicide rates during and after the COVID-19 outbreak. Our study suggests that unemployment is a factor that negatively affects mental health. Previous studies have shown that long working hours are associated with an increased risk of depression in Japan. Similar results were obtained in the multiple regression analysis [23].
Table 1: Baseline Characteristics Before and After Propensity Score Matching
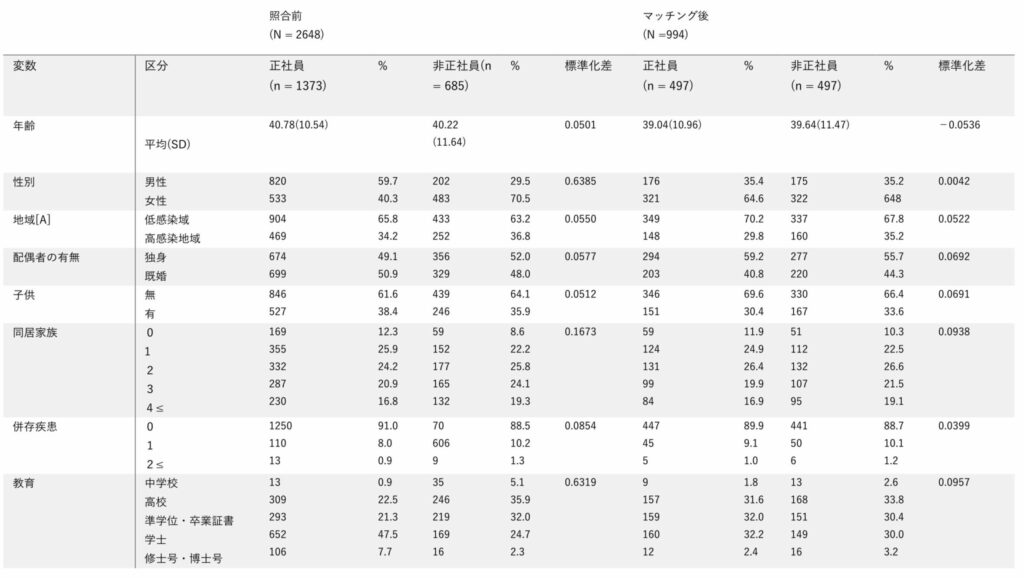
CES-D = Center for Epidemiologic Studies Depression Scale, SOC = Sense of Coherence, SD = Standard Deviation
[A] High infection areas include Tokyo, Saitama, Chiba, Kanagawa, and Hokkaido.
[B] Income levels are categorized as low (less than 4 million yen), medium (4 million to less than 8 million yen), and high (8 million yen or more).
[C] Exercise is defined as moderate activity for about an hour with light breathing.
[D] Industries are classified as follows: primary industries including agriculture, forestry, and fisheries; secondary industries including mining, quarrying, construction, and manufacturing; tertiary industries including electricity, gas, heat supply, water supply, information and communication, transportation and postal services, wholesale and retail trade, finance and insurance, real estate and rental services, scientific research, professional and technical services, accommodation, food services, personal and amusement services, education and learning support, healthcare and welfare, combined services, other services, government, and unclassifiable industries.
Figure 3: Box Plots of Changes in CES-D Scores and Health-Related Utility, and Background Diagrams of Unemployment Experience in the Persistent and Non-Persistent Groups
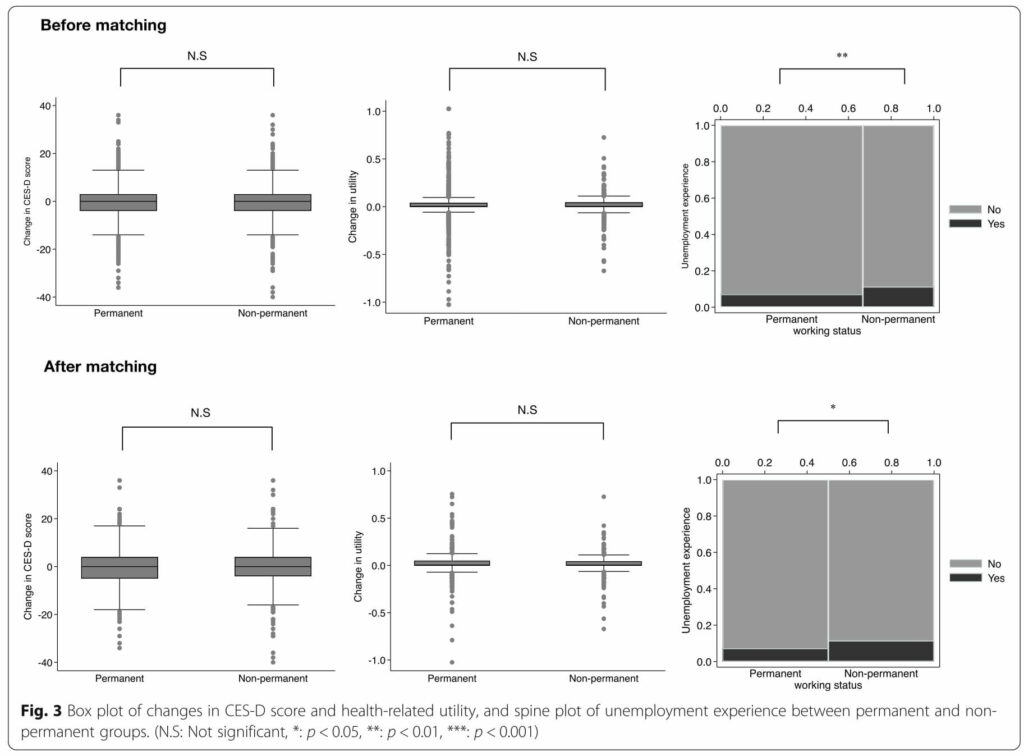
Before Matching = 照合前, After Matching = 照合後, Change in CES-D = CES-Dスコアの変化, Change in utility = 効用の変化, Unemployment experience = 失業経験, Permanent = 永久, Non-employment = 非常勤, working status = 稼動状況
Twenge et al. [24] reported that the prevalence of depression in the United States slightly increased from April to May 2020. The prevalence of diagnosed depression could not be estimated. However, half of the subjects in this data confirmed depressive symptoms, as indicated by CES-D scores of 16 points or more. Therefore, this is not an optimal situation, and the increase in unemployment may lead to an increased incidence of depression in Japan in the near future.
Web-based surveys are a reliable method for epidemiological research [25, 26]. However, this study had several limitations. First, due to the inability to obtain a second response from the web survey, about 25% of the subjects were excluded from the follow-up survey. Younger participants were more likely to be non-responsive to the follow-up survey. Therefore, some selection bias remained regarding the follow-up data compared to the initial survey data. However, such selection bias likely had minimal impact on our results as sufficient representation of the Japanese population was ensured in the initial survey. Second, this study targeted workers employed by commercial enterprises, so self-employed individuals and public servants were excluded from the analysis. Public servants are considered to be engaged in public duties, and self-employed individuals generally work independently. Due to the limited number of subjects in the follow-up data, further data collection is necessary in future studies to investigate the mental health status of workers.
Finally, in the follow-up survey questionnaire, unemployment was defined as job loss or dismissal during the state of emergency. More information about the reasons for unemployment could not be collected. Additionally, it was impossible to use additional approaches to verify the respondents' socioeconomic status or clinical history due to the anonymous self-report nature of the survey. Despite these limitations and the short-term prospective survey, the statistical analysis presented in this study could serve as important information for future health and economic policies related to the COVID-19 crisis in Japan.
After the state of emergency declaration, the Japanese government encouraged citizens to refrain from unnecessary travel and to avoid going out except when necessary. The closure of many public and commercial facilities was strongly urged except for essential businesses. Although mandatory measures such as lockdowns were not implemented in other countries, most people exercised self-restraint until the emergency was lifted. Japan successfully controlled the virus by the end of June. However, according to the Ministry of Health, Labour and Welfare [27, 28], the number of unemployed due to COVID-19 was estimated at 48,206 as of August 25. Japan is facing a second wave of COVID-19, and the situation is likely to remain severe in the medium to long term. Increased unemployment rates are expected in specific industries such as manufacturing, food service, and tourism. Therefore, changes in mental health and suicide rates should be carefully monitored.
Table 2: Multiple Regression Model of Socioeconomic Indicators and Changes in CES-D Scores (N = 2351)
|
Variable |
Coefficient |
95% CI Lower |
95% CI Upper |
P Value |
|
Part-time |
0.135 | -0.720 | 0.989 | 0.757 |
|
Unemployment Experience |
2.358 | 0.793 | 3.923 | 0.003 |
|
Non-regular Employment * Unemployment Experience |
-1.148 | -3.507 | 1.210 | 0.340 |
|
Gender |
-0.301 | -1.055 | 0.452 | 0.433 |
|
Age |
-0.015 | -0.050 | 0.020 | 0.397 |
|
Number of Comorbidities |
1.000 0.939 3.284 0.566 -0.821 |
-0.238 0.092 -0.125 -1.570 |
2.116 6.476 1.256 -0.072 |
0.118 0.044 0.108 0.032 |
|
Personal Income |
1.000 -0.078 -0.551 |
-1.122 -2.099 |
0.967 0.998 |
0.884 0.486 |
|
Household Income |
1.000 -0.465 -1.003 |
-1.417 -2.189 |
0.486 0.184 |
0.338 0.098 |
|
Average Daily Working Hours |
1.000 -0.091 1.574 0.467 |
-0.888 0.179 -2.210 |
0.706 2.969 3.145 |
0.822 0.027 0.732 |
| Union Member | -0.194 | -0.928 | 0.540 | 0.604 |
| Household Head | 0.235 | -0.617 | 1.087 | 0.589 |
|
Exercise Once every two weeks |
1.000 0.531 0.537 -0.203 |
-0.639 -0.472 -1.126 |
1.701 1.545 0.719 |
0.373 0.297 0.665 |
|
Smoking |
1.000 -0.604 0.011 |
-1.151 -1.441 |
0.611 0.766 |
0.548 0.548 |
|
Drinking |
1.000 -0.604 0.011 |
-1.306 -1.527 |
0.097 1.549 |
0.091 0.989 |
|
Sleep Duration |
0.750 -0.052 1.000 0.999 |
-1.381 -0.838 |
2.880 0.735 |
0.490 0.898 |
| SOC Score | -0.134 | -0.172 | -0.097 | <0.001 |
|
Baseline CES-D Score |
-0.383 | -0.420 | -0.347 | <0.001 |
|
Constant |
14.721 | 11.913 | 17.528 | <0.001 |
CES-D = Center for Epidemiologic Studies Depression Scale, SOC = Sense of Coherence
*: P < 0.05, **: P < 0.01, ***: P < 0.001
Conclusion
In conclusion, this study found that the mental health of non-regular workers was not adversely affected by the state of emergency due to COVID-19 in Japan. The authors suggest that a history of unemployment is a factor associated with a decline in mental health, and about 10% of non-regular workers experienced unemployment during the two periods. The COVID-19 crisis is still in its early stages, and systematic policies, including infection control and economic measures, are necessary to prevent the deterioration of mental health among general workers. Further research is needed to assess the long-term mental health outcomes and the incidence of depression during the COVID-19 crisis in Japan.
Abbreviations
OECD: Organisation for Economic Co-operation and Development
DSM-5: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
HRQOL: Health-Related Quality of Life
CES-D: Center for Epidemiologic Studies Depression Scale
SOC: Sense of Coherence
References
1. World Health Organization. Coronavirus disease 2019 (COVID-19) Situation; 2020. p. 196. https://www.who.int/emergencies/diseases/novel-corona virus-2019/situation-reports. Accessed on 7 August, 2020
2. Organization for Economic Co-Operation and Development (OECD). Record rise in OECD unemployment rate in April 2020. (2020) http://www.oecd.org/ sdd/labour-stats/unemployment-rates-oecd-update-june-2020.htm . Accessed on 27 August, 2020. Table 2 Multiple linear regression models of socioeconomic indicators and changes in the CES-D score (N = 2351) (Continued) Variables Coefficient Lower 95% CI Upper 95% CI P value SOC score −0.134 −0.172 − 0.097 < 0.001 *** Base-line CES-D score −0.383 −0.420 − 0.347 < 0.001 *** Constant 14.721 11.913 17.528 < 0.001 *** CES-D Center for Epidemiologic Studies Depression Scale, SOC Sense of coherence *: P < 0.05, **: P < 0.01, ***: P < 0.001
3. Looi MK. Covid-19: Japan prepares to extend state of emergency nationwide as “untraceable” cases soar. BMJ. 2020a;369:m1543. https://doi. org/10.1136/bmj.m1543.
4. Looi MK. Covid-19: Japan declares state of emergency as Tokyo cases soar. BMJ. 2020b;369:m1447. https://doi.org/10.1136/bmj.m1447.
5. Shi L, Lu ZA, Que JY, Huang XL, Liu L, Ran MS, et al. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the coronavirus disease 2019 pandemic. JAMA Netw Open. 2020;3(7):e2014053. https://doi.org/10.1001/jamanetworkopen.2 020.14053.
6. González-Sanguino C, Ausín B, Castellanos MÁ, Saiz J, López-Gómez A, Ugidos C, et al. Mental health consequences during the initial stage of the 2020 coronavirus pandemic (COVID-19) in Spain. Brain Behav Immun. 2020; 87:172–6. https://doi.org/10.1016/j.bbi.2020.05.040. 7. López-Bueno R, Calatayud J, Ezzatvar Y, Casajús JA, Smith L, Andersen LL, et al. Association between current physical activity and current perceived anxiety and mood in the initial phase of COVID-19 confinement. Front Psychiatry. 2020;11:729. https://doi.org/10.3389/fpsyt.2020.00729.
8. Ueda M, Stickley A, Sueki H, Matsubayashi T. Mental health status of the general population in Japan during the COVID-19 pandemic. Psychiatry Clin Neurosci. 2020. https://doi.org/10.1111/pcn.13105.
9. Statistics Bureau. Ministry of Internal affairs and communications, Labour Force Survey monthly results. (2020) http://www.stat.go.jp/data/roudou/ sokuhou/tsuki/pdf/gaiyou.pdf. Accessed on June 2020 (Japanese).
10. Kachi Y, Otsuka T, Kawada T. Precarious employment and the risk of serious psychological distress: a population- based cohort study in Japan. Scand J Work Environ Health. 2014;40(5):465–72. https://doi.org/10.5271/sjweh.3442.
11. Jang SY, Jang SI, Bae HC, Shin J, Park EC. Precarious employment and newonset severe depressive symptoms: a population-based prospective study in South Korea. Scand J Work Environ Health. 2015;41(4):329–37. https://doi. org/10.5271/sjweh.3498.
12. Yoo KB, Park EC, Jang SY, Kwon JA, Kim SJ, Cho KH, et al. Association between employment status change and depression in Korean adults. BMJ Open. 2016;6(3):e008570. https://doi.org/10.1136/bmjopen-2015- 008570.
13. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. 2016;387(10024): 1227–39. https://doi.org/10.1016/S0140-6736(15)00234-2.
14. Ina K, Hayashi T, Nomura H, Ishitsuka A, Hirai H, Iguchi A. Depression, quality of life (QoL) and will to live of community-dwelling postmenopausal women in three Asian countries: Korea, China and Japan. Arch Gerontol Geriat. 2011;53(1):8–12. https://doi.org/10.1016/j.archger.2010.05.010.
15. Kuroki T, Ishitobi M, Kamio Y, Sugihara G, Murai T, Motomura K, et al. Current viewpoints on DSM-5 in Japan. Psychiatry Clin Neurosci. 2016;70(9): 371–93. https://doi.org/10.1111/pcn.12421.
16. Ohta M, Higuchi Y, Yamato H, Kumashiro M, Sugimura H. Sense of coherence modifies the effect of overtime work on mental health. J Occup Health. 2015;57(3):297–301. https://doi.org/10.1539/joh.14-0164-BR.
17. Lewinsohn PM, Seeley JR, Roberts RE, Allen NB. Center for Epidemiologic Studies Depression Scale (CES-D) as a screening instrument for depression among community-dwelling older adults. Psychol Aging. 1997;12(2):277–87. https://doi.org/10.1037/0882-7974.12.2.277. 18. Shiroiwa T, Ikeda S, Noto S, Igarashi A, Fukuda T, Saito S, et al. Comparison of value set based on DCE and/or TTO data: scoring for EQ-5D-5L health states in Japan. Value Health. 2016;19(5):648–54. https://doi.org/10.1016/j.jva l.2016.03.1834.
19. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. https://doi.org/10.1080/00273171.2011.568786.
20. Sairenchi T, Haruyama Y, Ishikawa Y, Wada K, Kimura K, Muto T. Sense of coherence as a predictor of onset of depression among Japanese workers: a cohort study. BMC Public Health. 2011;11(205):205. https://doi.org/10.11 86/1471-2458-11-205.
21. Urakawa K, Yokoyama K, Itoh H. Sense of coherence is associated with reduced psychological responses to job stressors among Japanese factory workers. BMC Res Notes. 2012;5(247):247. https://doi.org/10.1186/1756-0500- 5-247.
22. Kikuchi H, Odagiri Y, Ohya Y, Nakanishi Y, Shimomitsu T, Theorell T, et al. Association of overtime work hours with various stress responses in 59,021 Japanese workers: retrospective cross-sectional study. PLoS One. 2020;15(3): e0229506. https://doi.org/10.1371/journal.pone.0229506.
23. Nakata A. Long working hours, job satisfaction, and depressive symptoms: a community-based cross-sectional study among Japanese employees in small- and medium-scale businesses. Oncotarget. 2017;8(32):53041–52. https://doi.org/10.18632/oncotarget.18084.
24. Twenge JM, Joiner TE. U.S. Census Bureau-assessed prevalence of anxiety and depressive symptoms in 2019 and during the 2020 COVID-19 pandemic. Depress Anxiety. 2020. https://doi.org/10.1002/da.23077.
25. Smith B, Smith TC, Gray GC, Ryan MA. Millennium cohort study team. When epidemiology meets the internet: web-based surveys in the millennium cohort study. Am J Epidemiol. 2007;166(11):1345–54. https://doi.org/10.1 093/aje/kwm212.
26. Ekman A, Dickman PW, Klint A, Weiderpass E, Litton JE. Feasibility of using web-based questionnaires in large population-based epidemiological studies. Eur J Epidemiol. 2006;21(2):103–11. https://doi.org/10.1007/s10654- 005-6030-4.
27. Ministry of Health, Labour and Welfare. Employment Security. (2020) https:// www.mhlw.go.jp/english/policy/employ-labour/employment-security/index. html . Accessed on 27 August, 2020.
28. Japan Institute for Labour Policy and Training. Results of the “Survey on the Impact that Spreading Novel Coronavirus Infection has on Work and Daily Life.” (2020) https://www.jil.go.jp/english/index.html . Accessed on 27 August, 2020.